A review of statin use for the prevention of cardiovascular disease shows very positive support for the use of statin medication. My readers know that I am very much in favor of lifestyle changes to lower cardiovascular risk and this is always the preferred first strategy. This just published article validates the safety and net benefit of medication in the event a person’s risk is not optimal. Contrary to much lay literature the science on this is very strong. Read the study abstract for complete information. I felt as a bottom line comment to the readers an excerpt from the article is very important to note.
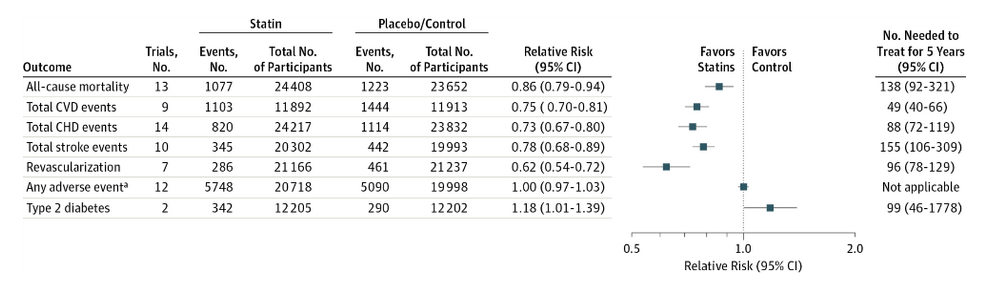
“The incidence of cancers, myalgia, rhabdomyolysis, liver enzyme elevation, renal dysfunction, or arthritis did not differ between the groups, although not all trials reported fully on these outcomes. Rates of adverse events (17%) and stopping treatment (12%) were similar in statin and placebo/control groups.”
Bottom line here: A large and mature body of literature (and my clinical experience) supports all-cause mortality benefit from the use of statin therapy for persons at risk for heart attack, large vessel atherosclerosis and stroke. If all-cause mortality is reduced, this by definition means subjects using medication are not trading a heart attack for fatal liver disease (a myth), or cancer induced by the medication. If you need it, you should feel comfortable taking it.
what about those few people who suffer side effects(muscular problems and liver damage). Never a problem for me after 25 years of use but have friends who have had both problems
Don Scott
According to the study referenced, such side effects were equal to the placebo group. Liver enzyme elevations in lab work sometimes occur but are usually mild and go away with ongoing therapy. There are drug interactions with other medications that might stress liver function and require a reassessment of a patient’s drug regimen. I’ve actually seen prescription strength niacin cause more significant liver enzyme elevations than statin therapy alone.
18% increase in T2 outcome jumps off the page, am I reading that right? This seems to indicate a tight-rope balancing act when it comes to preventative strategies. What if a patient has no signs of CVD but has elevated lipids, at what point do we elevate the risk of T2 in the name of possible atheroma prevention? Should statins be a part of an integrative prevention paradigm even in asymptomatic patients with no known plaque burden?