Other possible titles are: ” Ode to the Last of the Hold-outs” or “Woe is Me, The Doctor of Yesteryear”or ” How I Don’t Love You Doctor- Let Me Count The At Least 18 Ways”
My son who works for one of the largest banks in the country, recently shared with me an analysis carried out regarding private medical practices. In the past 10 years, the number of privately owned and operated physician practices has gone from over 80% to now just under 28%! That is a massive shift in the work force and potentially in customer service and patient interests since doctors have traditionally been the advocates for their patients.
Doctors have traditionally tried to keep all other parties out of the examination room unless those invited were going to help our patients. It appears in the past 10 years we are experiencing a collaborative effort to have your doctor working for someone besides yourself, the patient. Under Medicare we are working for the government. Since Obamacare the conflict of interest is to look at each patient as a cost liability. That is all you hear about in the political sphere. Some of my physician lobbies (ie AMA and ACP) have been complicit in this shift of priorities. Each time these lobbies give you, the patient, up in the discussion they are misguided. Policies promoting placing us physicians into hospital and corporate employment arrangements sacrifices the patient doctor relationship by introducing conflicts of interest. It further shifts the balance of power away from the patient buyer to some administrative and costly entity.
This calendar year I decided to move into solo private practice from group practice. My instincts tell me that rapid, adaptive decision making will be necessary to stay independent of conflicts of patient interest as further health regulation unfolds. As a fierce patient advocate and president of our Independent Physician Association (see www.ipalc.org), I have been taking an inventory of many (this list doesn’t include all) of the forces working against the patients, especially Medicare patients. Following is a rundown.
- Automatic Medicare enrollment from birth for any newly licensed doctor. Regardless of speciality (including Pediatrics) your physician is counted as a Medicare provider unless she or he actively opts out of Medicare. This is passive coercion.
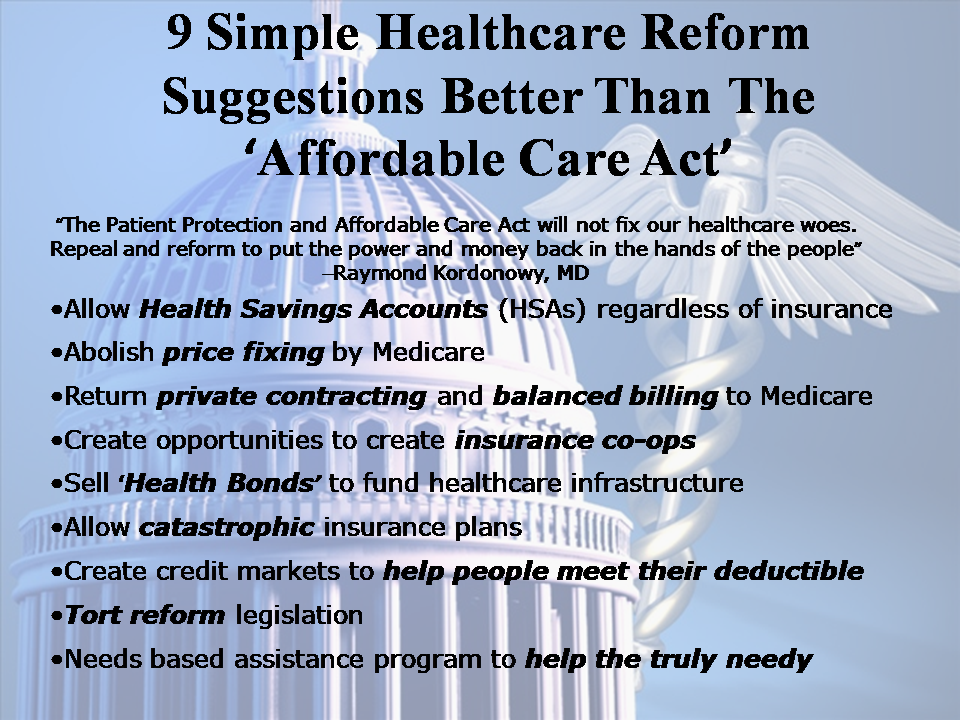
- Medicare Price-fixing physician services-making it illegal for doctors to collect payment over the set fees schedule. No contracting period is offered, each January the prices are announced.
- Opting out of Medicare is an active process that involves a 2 year period of no involvement along with a documented patient notice contract and no payment of any kind allowed to the patient nor the opted out doctor for services rendered. Does this sound coercive?
- Private insurance payments are indexed against the Medicare fixed fee schedule. It is a myth that private insurance is carrying Medicare’s lower payment. The reality is the insurance companies are forcing payment to at or below Medicare. The reasoning is simple and perpetuated by Medicare price-fixing. Why pay more if the doctor will accept the Medicare fee schedule? So far most doctors have not left the Medicare program and so this position is reinforced.
- Ever rapidly rising and arbitrary costly regulatory mandates force more doctor and staff hours to provide the same services-productivity is dropping. The electronic prescribing and electronic health record requirements are examples. This October a whole new coding system called ICD 10 will be required. This will place at least 25% of claims in denial, reduce charge entry productivity at least 15% thus ensuring a cash flow crisis in the private doctor’s office.
- Price cuts and fixing are making it financially impossible to provide common services (examples are osteoporosis treatment and even bone density testing)
- Increasing Medicare payment denials and various strategies by the program to get “free” care from any efficiency produced. Examples are paying for only one service during an encounter where more than one service was provided.
- Random/arbitrary claims denials by Medicare and insurance companies- this hurts cash flow and raises operating overhead, not to mention harming office and doctor moral.
- The Medicare claims system has barriers in place including automatic claim denials based upon the service or diagnosis code used.
- Patients lack understanding regarding insurance products and contract changes- causing payment complaints and questions directed to the office. Your doctor’s office isn’t an insurance claims arbitration unit.
- Dealing with prescription denials- even generic medications-and the ensuing additional physician and nurse chart reviews and clerical work forced back into the office, after your visit encounter.It comes from your insurance plan denying you services but results in your doctor being forced to advocate on your behalf- she or he becomes the dumping ground for this decision. It happens several times a day in any medical office. This is another example of getting additional “free” services from your provider while the insurance carrier and prescription benefits manager makes more profit from your monthly payments. These maneuvers add work after the visit with no compensation unless your doctor invoices you privately (a practice I presently use).
- Medicare and the secondary insurance carriers are denying payment while asking for more chart documentation to prove the truth of patient treatment during a visit.
- Mandated physician order oversight signatures from virtually any outside medical supply or therapy referral as well as retirement living facilities. I am now asked to sign orders for over the counter medications for clients who live in Senior living apartments. No one pays for this legal risk and additional administrative work.
- Mandated regulatory changes adding to practice overhead- with no ability to change office prices for Medicare patients unless the doctor quits Medicare. If a doctor quits Medicare, patients then can’t get any reimbursement for services paid for in the doctors office.
- Future penalties to practices that fail to comply with regulatory requirements starting this year (2014).
- Due to regulated price policies difficulty in getting patients referrals/access and even medications. We have been having shortages of even the most basic IV fluids.
- The New 2014 MACRA law is extending price-fixing an additional 5 years with plans to “restructure” physician and practice payment method- all while mandating further “to yet be defined” quality measure requirements and additional regulatory and bureaucratic policies. Who will be policing this is also to be determined.
- Hourly risk for “claims fraud” due the impossible documentation requirements that exist in the Medicare services codes as well as oversight policies. One biased audit could devastate any practicing doctor.
